A pediatrician and a computer scientist are creating a powerful tool to save young lives in large-scale emergencies.
“Pediatric disaster victims present unique problems,” says the physician, Jeffrey S. Upperman M.D. of Childrens Hospital Los Angeles. “Children cannot be treated simply as miniature adults. Children have special needs. Some are seemingly trivial — stockpiling smaller equipment and appropriate pharmaceutical dosages, and some are more demanding. Most important of all: an adult can be treated at an emergency center and told to go home, a child cannot.” Upperman and his collaborator, Robert Neches of the USC Information Sciences Institute, believe that in the confusion following a large earthquake or other major disaster, the lives of children will depend on ways to get the latest, best information about resources and needs into the hands of decision makers, quickly, accurately, and flexibly, in a form that enables them to make the right moves.
Upperman and his collaborator, Robert Neches of the USC Information Sciences Institute, believe that in the confusion following a large earthquake or other major disaster, the lives of children will depend on ways to get the latest, best information about resources and needs into the hands of decision makers, quickly, accurately, and flexibly, in a form that enables them to make the right moves.
Neches, a division director at ISI who designs successful systems the military now uses to do precisely this, has been working with Upperman to adapt to emergency pediatrics the lessons learned from (for example) software he built that allows Marine corps air units to plan, quickly and effectively missions based on the latest information.
The project has the vision of establishing what the working paper calls “Comprehensive Information Technology Support for Pediatric Disaster Preparation and Response.”
“We saw in Katrina how the best-laid plans become dead letters unless decision makers have effective ways to continuously assess the situation and modify plans in timely and appropriate fashion,” said Neches. “Modern systems are emerging that have these capabilities. The problem is, so far they haven’t been adapted to this problem.”
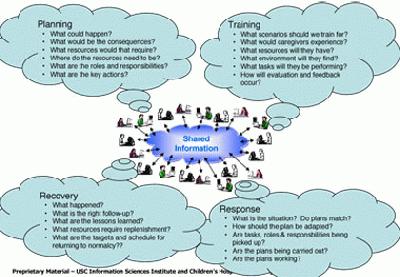
The model the partners are working on is called an “adaptive planning paradigm.”
“Adaptive planning breaks down the barriers between preparation and execution; it eliminates the dual problems of creating plans that are not followed and following plans that don’t fit,” explains Neches. “The key is the ability to speedily gather and assess information from a huge variety of sources, including real time sensors, and to package and disseminate results so plans can be executed – or changed.
Neches software in other applications, including one being developed for DARPA to aid combat commanders make decisions, creates a kind of parliament inside a computer in which each potential element (ambulances, hospitals, supplies, doctors, etc) gets a special subprogram that continuously monitors its particular domain, and communicates with its peers.
The plan rolls out by first modeling, in detail, existing conditions using known quantities: what resources are where. Next, researchers would integrating these facts into a virtual model like the ones used in the previous systems. Next, the priorities and “best-practice” rules developed over past emergencies would be embedded into the system, as similar rules for running air operations were embedded into Neches’ earlier systems. to Finally, researchers and potential users test the system, using simulated emergency situations to gauge the effectiveness of the system’s response.
Typical of the kind of problem analyzed and embedded into to the system is the critical issue of triage – knowing what medical needs are in the whole area, and prioritizing them. In a regional emergency, patients will be coming through multiple units and hospitals. Rather than have this process take place in isolation, the idea is to tie activities at all these centers together, connecting them via communications that remain working even in severe situations.
Pediatric triage focuses on the fact that most children who are seriously injured need respiratory support above all. “We envision decision-support software that will provide real-time data for pediatric disaster victims that present to a health care facility,” explains Upperman. “We believe that modern triage could be facilitated by a computer supported sensing system that allows hospital-based decision-makers an opportunity to direct time-sensitive resources to the appropriate children in the least amount of time.
To start with, as a model, the system will set up a “best practices” database that can both be accessed both by the machine modeling system and by individual human users, quickly offering accurate and timely suggestions.
The technology is now there, Neches says. “Systems that can help decision makers make accurate calls under heavy time pressure in crisis situations are a maturing but already useful technology. We think the time has come to put this technology to use to save children’s lives in pediatric emergencies.”
Neches and Upperman hope to begin work this fall, with funding from USC and other sources.
Published on July 19th, 2006
Last updated on August 9th, 2021